Eric H Kossoff, Huei-Shyong Wang DOI:10.4103/2319-4170.107152 PMID:23515147
Since their introduction in 1921, high-fat, low-carbohydrate "ketogenic" diets have been used worldwide for refractory childhood epilepsy. Approximately half of the children have at least half their seizures reduced, including 15% who are seizure free. The mechanisms of action of dietary therapies are under active investigation and appear to involve mitochondria. Once perceived as a last resort, modifications to initiation and maintenance, as well as the widespread use of pre-made ketogenic formulas have allowed dietary treatment to be used earlier in the course of epilepsy. For infantile spasms (West syndrome) specifically, the ketogenic diet is successful about 50% of the time as a first-line treatment. New "alternative" diets such as the modified Atkins diet were created in 2003 and can be started more easily and are less restrictive. They may have particular value for countries in Asia. Side effects include constipation, dyslipidemia, growth slowing, acidosis, and kidney stones. Additionally, neurologists are studying ketogenic diets for conditions other than epilepsy, including Alzheimer's disease, autism, and brain tumors.
Medium-chain Triglyceride Ketogenic Diet, An Effective Treatment for Drug-resistant Epilepsy and A Comparison with Other Ketogenic Diets
p. 9
Yeou-mei Christiana Liu, Huei-Shyong Wang DOI:10.4103/2319-4170.107154 PMID:23515148
The ketogenic diet (KD) is one of the most effective therapies for drug-resistant epilepsy. The efficacy of the medium-chain triglyceride KD (MCTKD) is as excellent as the classic KD (CKD), which has been documented in several subsequent retrospective, prospective, and randomized studies. MCT oil is more ketogenic than long-chain triglycerides. Therefore, the MCTKD allows more carbohydrate and protein food, which makes the diet more palatable than the CKD. The MCTKD is not based on diet ratios as is the CKD, but uses a percentage of calories from MCT oil to create ketones. There has also been literature which documents the associated gastrointestinal side effects from the MCTKD, such as diarrhea, vomiting, bloating, and cramps. Therefore, the MCTKD has been an underutilized diet therapy for intractable epilepsy among children.The author has used up to >70% MCTKD diet to maximize seizure control with gastrointestinal side effects optimally controlled. As long as health care professionals carefully manage MCTKD, many more patients with epilepsy who are not appropriate for CKD or modified Atkins diet or low glycemic index treatment will benefit from this treatment. A comparison between the MCTKD and other KDs is also discussed.
Ketogenic Diet: An Early Option for Epilepsy Treatment, Instead of A Last Choice Only
p. 16
Huei-Shyong Wang, Kuang-Lin Lin DOI:10.4103/2319-4170.107155 PMID:23515149
Ketogenic diet (KD) was usually tried as a last resort in the treatment of intractable epilepsy after failure of many antiepileptics and even epilepsy surgery. Glucose transporter-1 deficiency and pyruvate dehydrogenase deficiency must be treated with KD as the first choice because of inborn errors of glucose metabolism. Infantile spasms, tuberous sclerosis complex, Rett syndrome, Doose syndrome, Dravet syndrome, etc., appear to respond to KD, and it has been suggested by the international consensus statement to use KD early. We believe that all patients with epilepsy, except those with contraindicated situations such as pyruvate carboxylase deficiency, porphyria, β-oxidation defects, primary carnitine deficiency, etc., may try KD before trying other regimens.
Background: Diagnosis of external root resorption (ERR) cavities may be challenging, especially when no clinical signs are seen. Therefore, the aim of this study was to compare the efficacy of conventional intraoral film radiography, charge-coupled device (CCD) detector, photostimulable phosphor plate (PSP) detector, and cone beam computed tomography (CBCT) for the detection of ERR.
Methods: The study sample comprised 54 maxillary first premolars. Cavities were created by using a low-speed handpiece with round diamond burs of 1 mm in diameter. Digital and conventional radiographs were taken from each tooth. Three observers examined all images for the presence of resorption cavities. Data were statistically analyzed with the χ2 test. The reliability and degrees of agreement were also determined by the mean of Cohen's Kappa analysis.
Results: The differences between the imaging methods in correct detection of root resorption for all sizes were not significant. For locations of root resorption, significant differences were found between CBCT and other methods in the apical regions.
Conclusions: CBCT was only useful for detection of cavities located in the apical one-third of the root, compared to other digital or conventional methods.
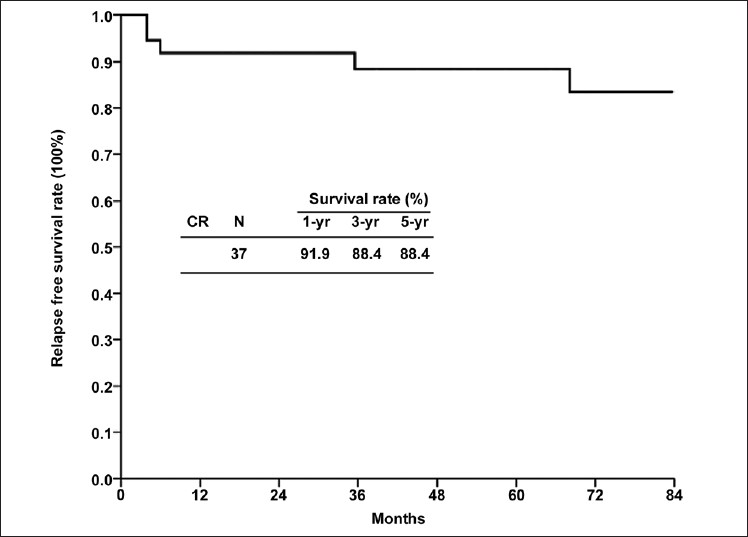
Background: Our aim is to identify the long-term relapse-free rate and predictive factors of response to splenectomy in adults with idiopathic thrombocytopenic purpura (ITP).
Methods: Between 1999 and 2005, 54 patients of ITP, who underwent splenectomy in Chang Gung Memorial Hospital, Linkou, Taiwan were retrospectively reviewed. Various pre, intra and postoperative factors were analyzed to determine the predictive factors of response and long-term disease-free rate after splenectomy in adult patients.
Results: The relapse free survival rates in complete response patients of splenectomy at 1-, 3- and 5-yr are 91.9%, 88.4%, and 88.4%, respectively. Younger age, response to steroids, pre- and postsplenectomy high platelet counts were found to be have significant p value of < 0.05 as predictive factors in univariate analysis. In multivariate analysis, only pre-op and post-op platelet counts were significant.
Conclusions: Significant long-term relapse-free survival rate is achieved by splenectomy in adults with ITP. In univariate analysis, age, response to steroids, pre- and postsplenectomy platelet counts were the significant predictive factors of response. But in multivariate analysis, only pre-op and post-op platelet counts were significant.
Impact of Extracorporeal Membrane Oxygenation Support on Clinical Outcome of Pediatric Patients with Acute Cardiopulmonary Failure: A Single-Center Experience
Background: Conventional therapy against acute pediatric cardiopulmonary failure (APCPF) caused by a variety of disease entities remains unsatisfactory with extremely high morbidity and mortality. For refractory APCPF, extracorporeal membrane oxygenation (ECMO) is one of the last resorts.
Methods: In this study, the in-hospital outcomes of pediatric patients with refractory APCPF receiving ECMO support were reviewed.
Results: Between August 2006 and May 2011, a single-center cohort study was performed in pediatric patients who required ECMO support due to cardiogenic shock or severe hypoxemia. A total of 22 patients with mean age of 7.0 ± 6.3 years received ECMO (male = 11; female = 11). The indications included acute fulminant myocarditis (AFM) (n = 6), congenital diaphragmatic hernia (CDH) (n = 3), acute respiratory distress syndrome (ARDS) (n = 6), enterovirus 71 (n = 3), viral sepsis (n = 2), refractory ventricular fibrillation due to long QT syndrome (n = 1), and pulmonary edema with brain herniation (n = 1). Eighteen patients received veno-arterial (VA) mode ECMO, while another four patients undertook the veno-venous (VV) mode. The duration of ECMO use and hospitalization were 6.1 ± 3.1 and 24.4 ± 19.4 days, respectively. The survival rate in patients with AFM was 100% (n = 6). Successful ECMO weaning with uneventful discharge from hospital was noted in 14 (63.6%) patients, whereas in-hospital mortality despite successful ECMO weaning occurred in 5 patients (22.7%). Failure in ECMO weaning and in-hospital death was noted in 3 patients (13.6%).
Conclusions: ECMO resuscitation is an effective strategy in the clinical setting of APCPF.
Background: Catatonia has risks of severe morbidity and mortality and needs early treatment. In this study, we investigated more patients to discuss the efficacy of this treatment in patients with major depressive disorder (MDD) or bipolar I disorder (BPI).
Methods: During a period of 9 years, we identified 12 catatonic patients with mood disorder, with MDD (n = 10) and BPI (n = 2) in the emergency department, inpatient and outpatient units of a general hospital. The patients received intramuscular injection (IMI) of 2 mg lorazepam once or twice during the first 2 h. If intramuscular lorazepam failed, intravenous dripping (IVD) of 10 mg diazepam in 500 mL normal saline every 8 h for 1 day was prescribed.
Results: Eight patients had full remission of catatonia after receiving one dose of 2 mg lorazepam IMI. Two patients needed two doses of 2 mg lorazepam IMI. Two patients with BPI recovered from catatonia using one dose of 10 mg diazepam IVD over 8 h after they failed to respond to two doses of 2 mg lorazepam IMI. The response rate to lorazepam IMI was 83.3%. All catatonic features remitted in 24 h with 100% response rate.
Conclusions: The lorazepam-diazepam treatment strategy is a safe and effective method to relieve catatonia in mood disorder within 1 day. Psychiatrist consultation is helpful for final diagnosis and rapid treatment of catatonia.