Activation-induced deaminase in B lymphocyte maturation and beyond
p. 259
Michel Cogné DOI:10.4103/2319-4170.113191 PMID:24385067
Activation-induced deaminase (AID), a member of the AID/apolipoprotein B mRNA-editing enzyme-catalytic (APOBEC) family, deaminates DNA cytidines into uridines and is the major trans-acting player of immunoglobulin (Ig) genes' diversification in mature B lymphocytes. It allows multiple antigen-driven Ig modifications through gene conversion and/or somatic hypermutation of variable region genes and also permits to switch from IgM expression to other antibody classes after class switch recombination, or to stop Ig expression after locus suicide recombination. AID is expressed at high levels into germinal center activated B cells with a very stringent temporal and spatial regulation. Despite multiple levels of regulation, off-target effects of AID are quite frequent in the B cell lineage and can affect a number of non-Ig genes, albeit at lower level than Ig genes. Beyond the immune system, AID also contributes to cytosine demethylation in undifferentiated cells by deaminating methylcytosines into thymines which are further processed by thymidine glycosylase. This contributes to the maintenance of pluripotency and to the limitation of genetic imprinting. Since AID attacks on DNA can induce replication errors, base excision repair, or mismatch repair, they are strongly mutagenic and are also driving forces of tumorigenesis, not only in B cell malignancies but also in some non-lymphoid tumors involving ectopic AID expression.
The inflammation amplifier, a nuclear factor-kappa B (NF-kB)feedback loop in non-immune cells including fibroblasts and endothelial cells, describes how NF-kB-mediated transcriptions are enhanced to induce the inflammation in the presence of signal Tranducer and Activator of Transcription 3 (STAT3) activation. It was originally discovered in rheumatoid arthritis and multiple sclerosis mouse models and has since been shown to be associated with various human diseases and disorders including autoimmune diseases, metabolic syndromes, neurodegenerative diseases, and other inflammatory diseases. The amplifier begins with IL-17, which acts as the main signal to express NF-kB-mediated transcriptions, and IL-6, an NF-kB target, which functions as a fuel for the inflammation amplifier. Indeed, other NF-kB targets including various chemokines also act as effector molecules that cause local accumulation of various immune cells and subsequent inflammation. Through extensive studies in the multiple sclerosis model experimental autoimmune encephalomyelitis, we recently demonstrated that regional neural activation induces excess activation of the inflammation amplifier at specific blood vessels in the fifth lumbar cord, creating a gateway for immune cells to enter the central nervous system (CNS). We thus propose the gateway theory to describe how regional neural activation enables immune cells to enter the CNS from the blood and argue that this theory might provide novel therapeutic targets for inflammatory diseases and disorders.
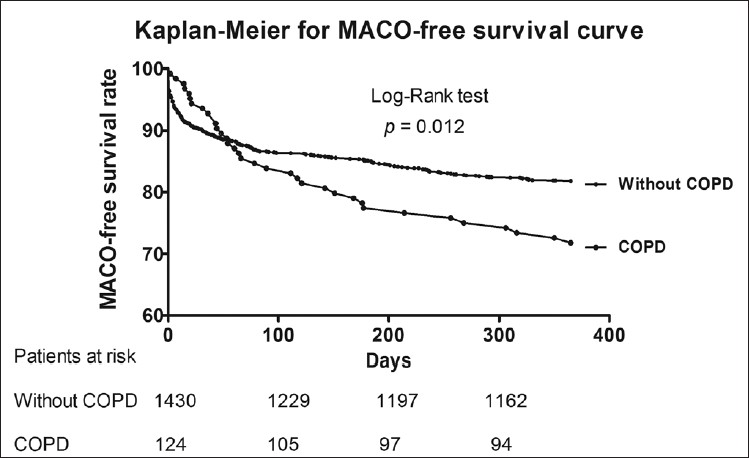
Background: This study reported the incidence and prognostic outcome of chronic obstructive lung disease (COPD) patients with acute ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI).
Methods: Between January 2002 and May 2011, totally 1554 consecutive patients who experienced STEMI undergoing primary PCI were enrolled into the study.
Results: Of the 1554 patients, 124 (9.7%) with diagnosis of COPD and 1430 (90.3%) without COPD were categorized into group 1 and group 2. Although no difference in in-hospital mortality was noted between the two groups (p = 0.726). However, the hospitalization duration was notably longer (p = 0.003), the incidences of recurrent MI and re-hospitalization for congestive heart failure were significantly higher in group 1 than in group 2 (all p < 0.02). Although Kaplan-Meier analysis demonstrated that the incidence of freedom from one-year major adverse clinical outcome (MACO) (defined as recurrent MI, re-admission for congestive heart failure was significantly lower in group 1 than group 2 (p = 0.012), multivariate Cox regression analysis showed COPD was not an independent predictor of MACO-free time after adjusting traditional risk factors.
Conclusion: COPD was not an independent predictor of short-term and medium-term MACO in patients with STEMI undergoing primary PCI.
Pulse pressure and michigan neuropathy screening instrument are independently associated with asymptomatic peripheral arterial disease among type 2 diabetes community residents: A community-based screening program in Taiwan
Background: Peripheral arterial disease (PAD) is one of the major manifestations of systemic atherosclerosis and plays an important role in low-extremity amputation in type 2 diabetic patients. The aim of this study was to explore the prevalence and risk factors for asymptomatic PAD in type 2 diabetic community residents.
Methods: This cross-sectional study enrolled 552 type 2 diabetic adults (232 men and 320 women) without subjective symptoms of intermittent claudication. We defined the PAD group as an ankle-brachial index (ABI) ≤ 0.90, and the normal group as an ABI 0.91-1.30. Their clinical characteristics, Michigan Neuropathy Screening Instrument (MNSI) scores and blood pressure were compared.
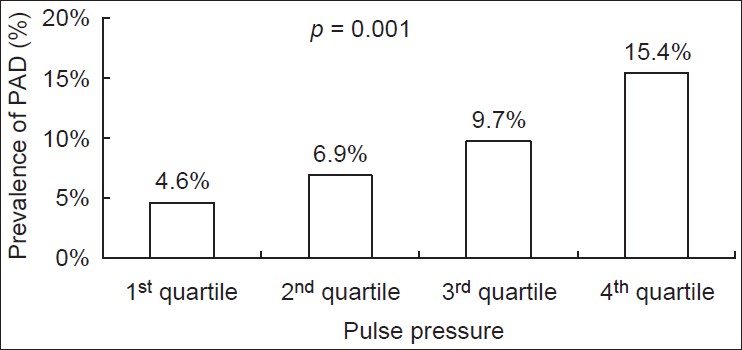
Results: We discovered that 51 patients have asymptomatic PAD. Univariate logistic regression analysis revealed that age, history of stroke, longer duration of diabetes (> 10 years), unemployment or retirement, pulse pressure, systolic blood pressure, and high MNSI score (> 2) were risk factors for PAD. By multivariate logistic regression analysis, pulse pressure, high MNSI score, age, and history of stroke were independent risk factors with odds ratios (95% confidence intervals, CI) of 1.032 (1.012-1.053), 2.359 (1.274-4.370), 1.050 (1.010-1.091), and 5.152 (1.985-13.368), respectively. Furthermore, the prevalence of PAD increased significantly with increment in the pulse pressure and MNSI.
Conclusions: In summary, the overall prevalence of asymptomatic PAD in the type 2 diabetic adults was 9.2%. Age, history of stroke, pulse pressure and MNSI score may provide important clinical information. Primary care physicians should be aware of asymptomatic patients with high pulse pressure and MNSI scores.
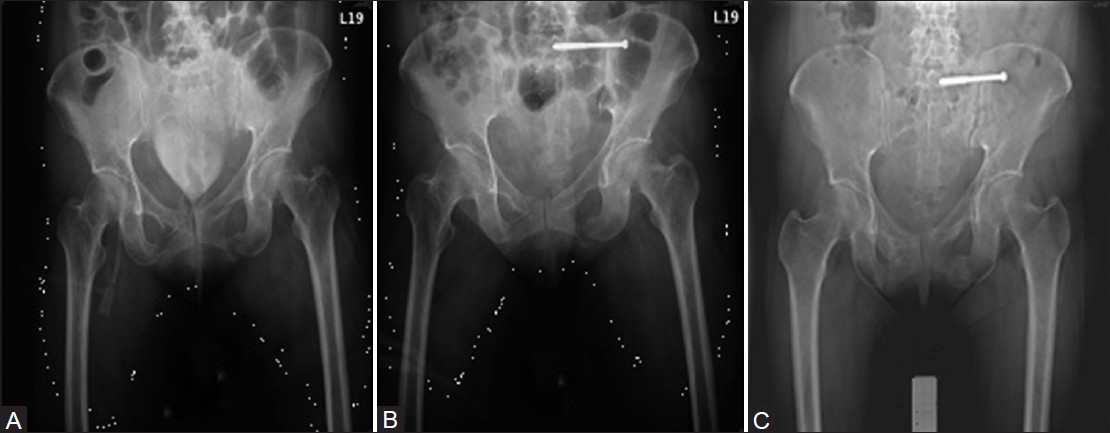
Background: Unstable posterior ring injuries of the pelvis are a challenge to pelvic surgeons, and their treatment has been controversial. The functional outcomes of such injuries following either percutaneous iliosacral screw fixation or conservative treatment remain to be elucidated.
Methods: We conducted a retrospective analysis of 32 consecutive patients with unstable pelvic ring injuries who were treated with percutaneous placement of iliosacral screws (group 1) or conservative means (group 2) from January 2002 to September 2009. Radiographic, clinical, and functional outcomes were compared between the two treatment groups.
Results: Patients who underwent percutaneous iliosacral screw fixation after pelvic trauma had better functional results than those treated conservatively, as per the Majeed grading system. In addition, patients in group 1 demonstrated better results for general health and mental health on the 36 item Short Form Health Status Survey. Patients in group 1 also demonstrated less residual displacement on radiography at 1 year follow up than those in group 2. Finally, patients in group 1 had better pain relief at 1 month and 1 year follow ups than those in group 2.
Conclusions: Percutaneous iliosacral screw fixation for unstable posterior pelvic ring injuries results in less residual displacement at medium term follow up, and better pain relief at short and medium term follow up, than does conservative treatment. Better functional outcomes were observed at 1 year follow up as compared with conservative treatment.
Background: Post-neurosurgical (post-NS) adult bacterial meningitis (ABM) with mixed infection is rarely examined solely in the literature.
Methods: The clinical features and laboratory data of post-NS ABM patients with mixed infection were included for analysis.
Results: Totally 170 post-NS ABM cases were identified and 18 (11 men and 7 women, aged 20-77 years, median = 57.5) of them had a mixed infection. A total of 45 bacterial strains including 34 Gram-negative [Gm(-)] strains and 11 Gram-positive [Gm(+)] strains were isolated. Of the implicated pathogens, Escherichia coli, Acinetobacter, Pseudomonas, and Klebsiella spp. were the common Gm(-) strains, while staphylococcal, streptococcal, and enterococcal strains were the common Gm(+) strains. Compared with the post-NS ABM cases with monomicrobial infection, those with mixed infection had a lower cerebrospinal fluid (CSF) white blood cell count. The mortality rate of post-NS ABM cases was 33.3% (6/18) without significant clinical and laboratory difference between the fatal and non-fatal groups.
Conclusion: Mixed infection is not uncommon in post-NS ABM (10.6%, 18/170), and its mortality rate is high. Seventy-six percent of the implicated bacterial pathogens belonged to Gm(-) strains, while the other 24% were Gm(+) strains. The clinical and laboratory features of ABM with mixed infection are not unique; its diagnosis can only be confirmed by a positive CSF culture.
Co-infusion of autologous adipose tissue derived insulin-secreting mesenchymal stem cells and bone marrow derived hematopoietic stem cells: Viable therapy for type III.C. a diabetes mellitus
p. 304
Umang G Thakkar, Aruna V Vanikar, Hargovind L Trivedi DOI:10.4103/2319-4170.122898 PMID:24385073
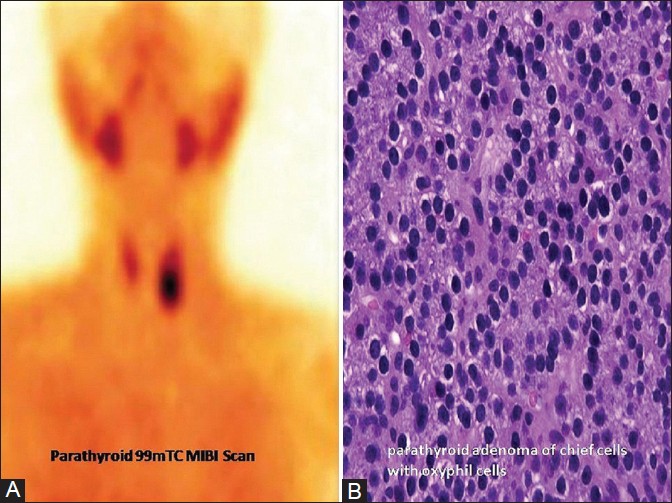
Transition from acute pancreatitis to insulin-dependent diabetes mellitus (IDDM) is a rare manifestation of primary hyperparathyroidism caused by parathyroid adenoma because of impaired glucose tolerance and suppresses insulin secretion. We report the case of a 26-year-old male with pancreatic diabetes caused by parathyroid adenoma induced chronic pancreatitis. He had serum C-peptide 0.12 ng/ml, glutamic acid decarboxylase antibody 5.0 IU/ml, and glycosylated hemoglobin (HbA1C) 8.9%, and required 72 IU/day of biphasic-isophane insulin injection for uncontrolled hyperglycemia. We treated him with his own adipose tissue derived insulin-secreting mesenchymal stem-cells (IS-ADMSC) along with his bone marrow derived hematopoietic stem cells (BM-HSC). Autologous IS-ADMSC + BM-HSC were infused into subcutaneous tissue, portal and thymic circulation without any conditioning. Over a follow-up of 27 months, the patient is maintaining fasting and postprandial blood sugar levels of 132 and 165 mg/dl, respectively, with HbA1C 6.8% and requiring 36 IU/day of biphasic-isophane insulin. Co-infusion of IS-ADMSC + BM-HSC offers a safe and viable therapy for type III.C.a Diabetes Mellitus.